Ankle Instability
What is Ankle Instability?
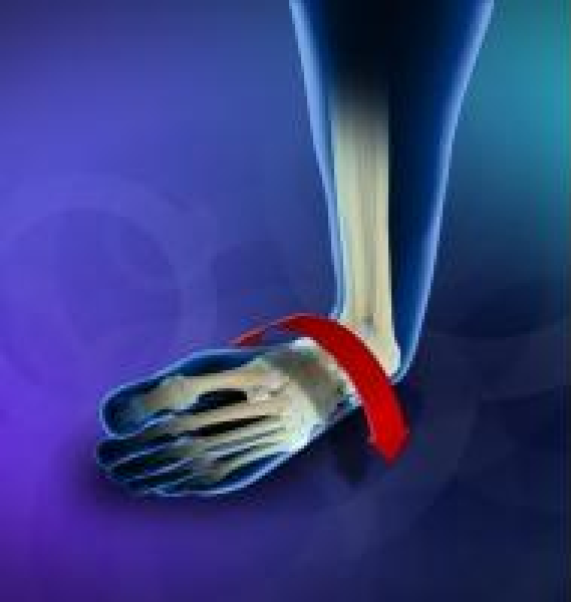
Ankle instability is a chronic condition characterised by a recurrent slipping of the outer side of the ankle. It usually results from repeated ankle sprains. It is generally noticed during movement of the ankle joint, but can also occur during standing.
Anatomy
The ankle joint is composed of three bones: the tibia, fibula and talus. The joint is protected by a fibrous membrane called a joint capsule, and filled with synovial fluid to enable smooth movement. Ankle stability is dependent on the ankle bones, and supporting ligaments and tendons. While the bones and ligaments provide static stability, dynamic stability is allowed by the tendons.
Causes of Ankle Instability
Repetitive injury of the ankle ligaments on the same side is the most common cause of ankle instability. Inadequate healing of the sprained ligament or incomplete rehabilitation of the affected ligament can result in instability of the ankle. Recurrent injury of the ligaments further weakens them and aggravates the instability, predisposing the development of additional ankle problems.
Symptoms of Ankle Instability
Pain is the most common symptom and is associated with swelling and tenderness of the ankle. There may be persistent discomfort and instability in the affected ankle joint. The ankle is unstable and may turn repeatedly while walking on uneven surfaces or during sports activity.
If Ankle Instability is Left Untreated
Left untreated, an unstable ankle joint significantly affects function and overall quality of living. It can eventually lead to chronic pain and arthritis.
Diagnosis of Ankle Instability
A complete medical history, including a history of any previous ankle injuries, and a physical examination is essential for an accurate diagnosis of the condition. An X-ray may be ordered to confirm the diagnosis. Other imaging tests may also be used to evaluate the injury.
Treatment of Ankle Instability
The management of ankle instability depends on the findings of the physical examination and the activity level of the patient.
Conservative Treatment
Conservative treatments include:
- Physiotherapy for improving the strength, balance and range of motion of the joint
- Bracing to support the affected ankle and prevent further sprain
- Non-steroidal anti-inflammatory drugs (NSAIDs) to reduce the pain and inflammation
Surgical Treatment
Surgery is recommended in patients with a high degree of instability and in those who have failed to respond to Nonsurgical treatments. Commonly used surgical procedures involve repair or reconstruction of the damaged ligament. There are two types of ankle instability surgery:
- Anatomic repair: involves shortening and tightening the stretched ligament
- Non-anatomic repair: uses a tendon as a graft to replace the damaged ligament
Conservative treatment is the first-line of treatment for ankle instability. Surgery is recommended in patients with a high degree of ankle instability and in those who have failed to respond to Nonsurgical treatments.
Anatomic repair is preferred in most cases of ankle instability.
Non-anatomic repair is performed in obese patients requiring increased stability or when tightening of the stretched and scarred ligaments is not strong enough, and needs to be reinforced with a tendon graft.
Procedure for Ankle Instability
There are two types of ankle instability surgeries:
Anatomic Repair
This involves reconstruction of the stretched or torn ligaments. Anatomic repair is preferred in most cases of ankle instability.
The surgery is performed under epidural anaesthesia. Your surgeon makes an incision on the ankle to expose the damaged joint and ligaments. The joint capsule and ligaments are examined, and the edges of the torn ligament are shortened and repaired with sutures. The ends may be overlapped and then sutured to strengthen the ligament. Your surgeon then covers the repaired ligament with the extensor retinaculum, a dense band of connective tissue, in order to reinforce the ligament further. Range of motion is evaluated, the incision is closed and a sterile bandage is applied.
Reconstructive Tenodesis
This is a tendon transfer procedure that uses your own or a cadaver tendon as a graft to replace the damaged tendon. Non-anatomic repair is performed in obese patients requiring increased stability or when tightening of the stretched and scarred ligaments is not strong enough and needs to be reinforced with a tendon graft.
The surgery is performed under epidural anaesthesia. Your surgeon makes an incision on your ankle. Drill holes are created where the damaged ligament normally attaches to the lower end of the fibula (calf bone) on one side and the talus (anklebone) on the other end. Your surgeon then harvests the peroneus brevis muscle tendon, found on the outer edge of the small toe, and weaves it through the drill holes to form a ligament complex. Range of motion is evaluated, the incision is closed and a sterile bandage is applied.
Post-Operation
After surgery, your foot will be immobilised with a cast or splint. You will be provided crutches to avoid bearing weight on the operated ankle. Your doctor will remove the splint and provide a removable boot to be worn for 2 to 4 weeks. Physiotherapy will be initiated to strengthen your joint and improve range of motion.
Outcomes
The outcome of surgery is based on the severity of the injury. In a few cases, instability may persist, requiring additional surgery. As with all surgical procedures, ankle instability surgery may be associated with certain complications including:
- Injury to the superficial nerves
- Chronic pain
- Stiffness
Downtime
Complete recovery may take 10 to 12 weeks.
Prognosis
The prognosis of ankle instability surgery is good if it has not been associated with arthritis because of chronic ankle instability that has caused the bones to rub against each other over many years.
Costs
Any costs involved will be discussed with you prior to your surgery.